Trump Administration Issues Second Round of
Sweeping Changes to Support U.S. Healthcare
System During COVID-19 Pandemic
At President Trump’s direction, and building on its recent historic efforts to help the U.S. healthcare system manage the 2019 Novel Coronavirus (COVID-19) pandemic, the Centers for Medicare & Medicaid Services today issued another round of sweeping regulatory waivers and rule changes to deliver expanded care to the nation’s seniors and provide flexibility to the healthcare system as America reopens. These changes include making it easier for Medicare and Medicaid beneficiaries to get tested for COVID-19 and continuing CMS’s efforts to further expand beneficiaries’ access to telehealth services.
CMS is taking action to ensure states and localities have the flexibilities they need to ramp up diagnostic testing and access to medical care, key precursors to ensuring a phased, safe, and gradual reopening of America.
Today’s actions are informed by requests from healthcare providers as well as by the Coronavirus Aid, Relief, and Economic Security Act, or CARES Act. CMS’s goals during the pandemic are to 1) expand the healthcare workforce by removing barriers for physicians, nurses, and other clinicians to be readily hired from the local community or other states; 2) ensure that local hospitals and health systems have the capacity to handle COVID-19 patients through temporary expansion sites (also known as the CMS Hospital Without Walls initiative); 3) increase access to telehealth for Medicare patients so they can get care from their physicians and other clinicians while staying safely at home; 4) expand at-home and community-based testing to minimize transmission of COVID-19 among Medicare and Medicaid beneficiaries; and 5) put patients over paperwork by giving providers, healthcare facilities, Medicare Advantage and Part D plans, and states temporary relief from many reporting and audit requirements so they can focus on patient care.
“I’m very encouraged that the sacrifices of the American people during the pandemic are working. The war is far from over, but in various areas of the country the tide is turning in our favor,” said CMS Administrator Seema Verma. “Building on what was already extraordinary, unprecedented relief for the American healthcare system, CMS is seeking to capitalize on our gains by helping to safely reopen the American healthcare system in accord with President Trump’s guidelines.”
Made possible by President Trump’s recent emergency declaration and emergency rule making, many of CMS’s temporary changes will apply immediately for the duration of the Public Health Emergency declaration. They build on an unprecedented array of temporary regulatory waivers and new rules CMS announced March 30 and April 10. Providers and states do not need to apply for the blanket waivers announced today and can begin using the flexibilities immediately. CMS also is requiring nursing homes to inform residents, their families, and representatives of COVID-19 outbreaks in their facilities.
New rules to support and expand COVID-19 diagnostic testing for Medicare and Medicaid beneficiaries
“Testing is vital, and CMS’s changes will make getting tested easier and more accessible for Medicare and Medicaid beneficiaries,” Verma said.
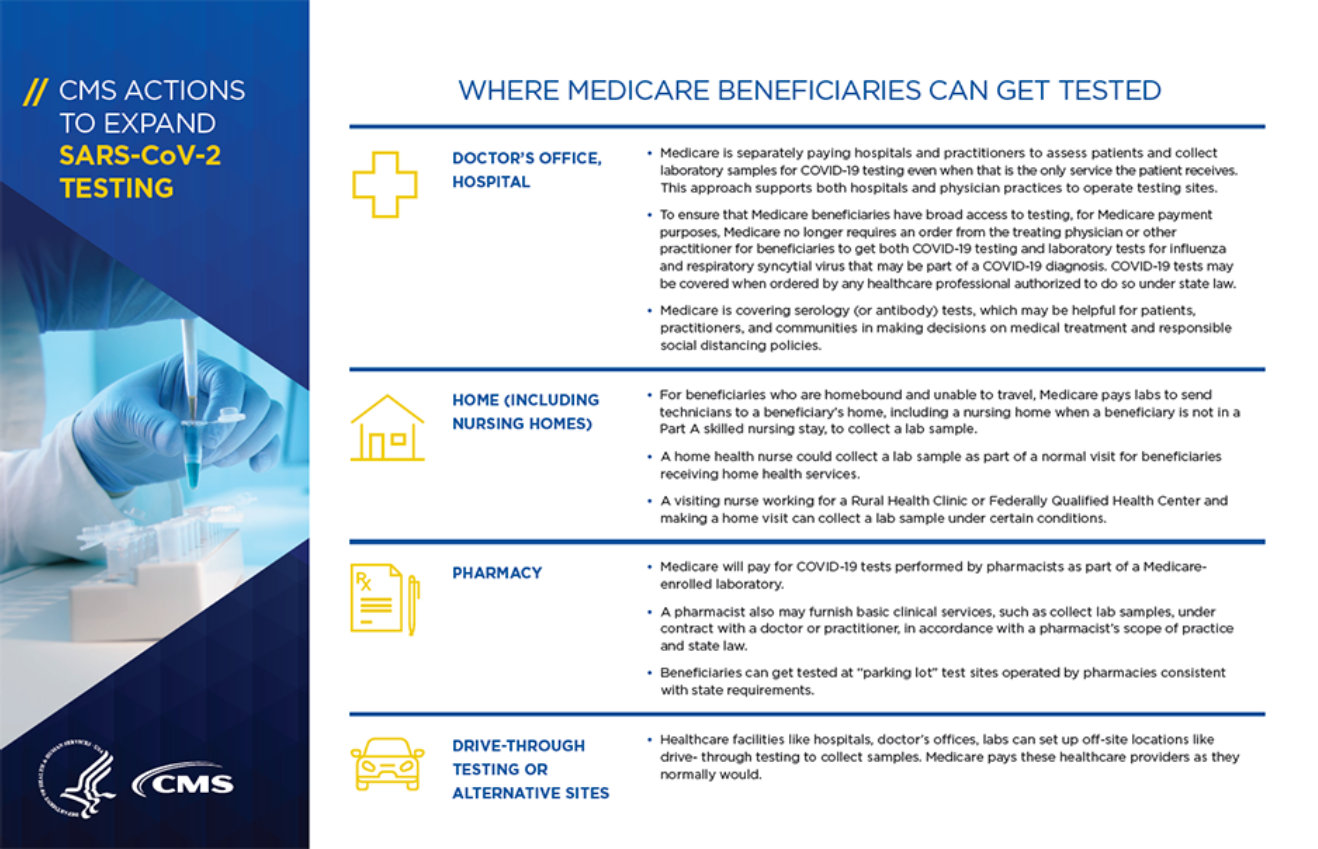
Under the new waivers and rule changes, Medicare will no longer require an order from the treating physician or other practitioner for beneficiaries to get COVID-19 tests and certain laboratory tests required as part of a COVID-19 diagnosis. During the Public Health Emergency, COVID-19 tests may be covered when ordered by any healthcare professional authorized to do so under state law. To help ensure that Medicare beneficiaries have broad access to testing related to COVID-19, a written practitioner’s order is no longer required for the COVID-19 test for Medicare payment purposes.
Pharmacists can work with a physician or other practitioner to provide assessment and specimen collection services, and the physician or other practitioner can bill Medicare for the services. Pharmacists also can perform certain COVID-19 tests if they are enrolled in Medicare as a laboratory, in accordance with a pharmacist’s scope of practice and state law. With these changes, beneficiaries can get tested at “parking lot” test sites operated by pharmacies and other entities consistent with state requirements. Such point-of-care sites are a key component in expanding COVID-19 testing capacity.
CMS will pay hospitals and practitioners to assess beneficiaries and collect laboratory samples for COVID-19 testing, and make separate payment when that is the only service the patient receives. This builds on previous action to pay laboratories for technicians to collect samples for COVID-19 testing from homebound beneficiaries and those in certain non-hospital settings, and encourages broader testing by hospitals and physician practices.
To help facilitate expanded testing and reopen the country, CMS is announcing that Medicare and Medicaid are covering certain serology (antibody) tests, which may aid in determining whether a person may have developed an immune response and may not be at immediate risk for COVID-19 reinfection. Medicare and Medicaid will cover laboratory processing of certain FDA-authorized tests that beneficiaries self-collect at home.
Additional highlights of the waivers and rule changes announced today:
Increase Hospital Capacity – CMS Hospitals Without Walls
Under its Hospitals Without Walls initiative. CMS has taken multiple steps to allow hospitals to provide services in other healthcare facilities and sites that aren’t part of the existing hospital, and to set up temporary expansion sites to help address patient needs. Previously, hospitals were required to provide services within their existing departments.
CMS is giving providers flexibility during the pandemic to increase the number of beds for COVID-19 patients while receiving stable, predictable Medicare payments. For example, teaching hospitals can increase the number of temporary beds without facing reduced payments for indirect medical education. In addition, inpatient psychiatric facilities and inpatient rehabilitation facilities can admit more patients to alleviate pressure on acute-care hospital bed capacity without facing reduced teaching status payments. Similarly, hospital systems that include rural health clinics can increase their bed capacity without affecting the rural health clinic’s payments.
CMS is excepting certain requirements to enable freestanding inpatient rehabilitation facilities to accept patients from acute-care hospitals experiencing a surge, even if the patients do not require rehabilitation care. This makes use of available beds in freestanding inpatient rehabilitation facilities and helps acute-care hospitals to make room for COVID-19 patients.
CMS is highlighting flexibilities that allow payment for outpatient hospital services — such as wound care, drug administration, and behavioral health services — that are delivered in temporary expansion locations, including parking lot tents, converted hotels, or patients’ homes (when they’re temporarily designated as part of a hospital).
Under current law, most provider-based hospital outpatient departments that relocate off-campus are paid at lower rates under the Physician Fee Schedule, rather than the Outpatient Prospective Payment System (OPPS). CMS will allow certain provider-based hospital outpatient departments that relocate off-campus to obtain a tem porary exception and continue to be paid under the OPPS. Importantly, hospitals may also relocate outpatient departments to more than one off-campus location, or partially relocate off-campus while still furnishing care at the original site.
Long-term acute-care hospitals can now accept any acute-care hospital patients and be paid at a higher Medicare payment rate, as mandated by the CARES Act. This will make better use during the pandemic of available beds and staffing in long-term acute-care hospitals.
Healthcare Workforce Augmentation:
To bolster the U.S. healthcare workforce amid the pandemic, CMS continues to remove barriers for hiring and retaining physicians, nurses, and other healthcare professionals to keep staffing levels high at hospitals, health clinics, and other facilities. CMS also is cutting red tape so that health professionals can concentrate on the highest-level work they’re licensed for.
Since beneficiaries may need in-home services during the COVID-19 pandemic, nurse practitioners, clinical nurse specialists, and physician assistants can now provide home health services, as mandated by the CARES Act. These practitioners can now (1) order home health services; (2) establish and periodically review a plan of care for home health patients; and (3) certify and re-certify that the patient is eligible for home health services. Previously, Medicare and Medicaid home health beneficiaries could only receive home health services with the certification of a physician. These changes are effective for both Medicare and Medicaid.
CMS will not reduce Medicare payments for teaching hospitals that shift their residents to other hospitals to meet COVID-related needs, or penalize hospitals without teaching programs that accept these residents. This change removes barriers so teaching hospitals can lend available medical staff support to other hospitals.
CMS is allowing physical and occupational therapists to delegate maintenance therapy services to physical and occupational therapy assistants in outpatient settings. This frees up physical and occupational therapists to perform other important services and improve beneficiary access.
Consistent with a change made for hospitals, CMS is waiving a requirement for ambulatory surgery centers to periodically reappraise medical staff privileges during the COVID-19 emergency declaration. This will allow physicians and other practitioners whose privileges are expiring to continue taking care of patients.
Put Patients Over Paperwork/Decrease Administrative Burden
CMS continues to ease federal rules and institute new flexibilities to ensure that states and localities can focus on caring for patients during the pandemic and that care is not delayed due to administrative red tape.
CMS is allowing payment for certain partial hospitalization services – that is, individual psychotherapy, patient education, and group psychotherapy – that are delivered in temporary expansion locations, including patients’ homes.
CMS is temporarily allowing Community Mental Health Centers to offer partial hospitalization and other mental health services to clients in the safety of their homes. Previously, clients had to travel to a clinic to get these intensive services. Now, Community Mental Health Centers can furnish certain therapy and counseling services in a client’s home to ensure access to necessary services and maintain continuity of care.
CMS will not enforce certain clinical criteria in local coverage determinations that limit access to therapeutic continuous glucose monitors for beneficiaries with diabetes. As a result, clinicians will have greater flexibility to allow more of their diabetic patients to monitor their glucose and adjust insulin doses at home.
Further Expand Telehealth in Medicare:
CMS directed a historic expansion of telehealth services so that doctors and other providers can deliver a wider range of care to Medicare beneficiaries in their homes. Beneficiaries thus don’t have to travel to a healthcare facility and risk exposure to COVID-19.
CMS previously announced that Medicare would pay for certain services conducted by audio-only telephone between beneficiaries and their doctors and other clinicians. Now, CMS is broadening that list to include many behavioral health and patient education services. CMS is also increasing payments for these telephone visits to match payments for similar office and outpatient visits. This would increase payments for these services from a range of about $14-$41 to about $46-$110. The payments are retroactive to March 1, 2020.
Hospitals may bill as the originating site for telehealth services furnished by hospital-based practitioners to Medicare patients registered as hospital outpatients, including when the patient is located at home.
Hospitals may bill for services furnished remotely by hospital-based practitioners to Medicare patients registered as hospital outpatients, including when the patient is at home when the home is serving as a temporary provider based department of the hospital. Examples of such services include counseling and educational service as well as therapy services. This change expands the types of healthcare providers that can provide using telehealth technology.
For the duration of the COVID-19 emergency, CMS is waiving limitations on the types of clinical practitioners that can furnish Medicare telehealth services. Prior to this change, only doctors, nurse practitioners, physician assistants, and certain others could deliver telehealth services. Now, other practitioners are able to provide telehealth services, including physical therapists, occupational therapists, and speech language pathologists.
CMS previously announced that Medicare would pay for certain services conducted by audio-only telephone between beneficiaries and their doctors and other clinicians. Now, CMS is broadening that list to include many behavioral health and patient education services. CMS is also increasing payments for these telephone visits to match payments for similar office and outpatient visits. This would increase payments for these services from a range of about $14-$41 to about $46-$110. The payments are retroactive to March 1, 2020.
As mandated by the CARES Act, CMS is paying for Medicare telehealth services provided by rural health clinics and federally qualified health clinics. Previously, these clinics could not be paid to provide telehealth expertise as “distant sites.” Now, Medicare beneficiaries located in rural and other medically underserved areas will have more options to access care from their home without having to travel
Since some Medicare beneficiaries don’t have access to interactive audio-video technology that is required for Medicare telehealth services, or choose not to use it even if offered by their practitioner, CMS is waiving the video requirement for certain telephone evaluation and management services, and adding them to the list of Medicare telehealth services. As a result, Medicare beneficiaries will be able to use an audio-only telephone to get these services.
In addition, CMS is making changes to the Medicare Shared Savings Program to give the 517 accountable care organizations (ACOs) serving more than 11 million beneficiaries greater financial stability and predictability during the COVID-19 pandemic.
ACOs are groups of doctors, hospitals, and other healthcare providers, that come together voluntarily to give coordinated high-quality care to their Medicare patients. The goal of coordinated care is to ensure that patients get the right care at the right time, while avoiding unnecessary duplication of services and preventing medical errors. When an ACO succeeds both in delivering high-quality care and spending healthcare dollars more wisely, it may share in any savings it achieves for the Medicare program.
Because the impact of the pandemic varies across the country, CMS is making adjustments to the financial methodology to account for COVID-19 costs so that ACOs will be treated equitably regardless of the extent to which their patient populations are affected by the pandemic. CMS is also forgoing the annual application cycle for 2021 and giving ACOs whose participation is set to end this year the option to extend for another year. ACOs that are required to increase their financial risk over the course of their current agreement period in the program will have the option to maintain their current risk level for next year, instead of being advanced automatically to the next risk level.
CMS is permitting states operating a Basic Health Program to submit revised BHP Blueprints for temporary changes tied to the COVID-19 public health emergency that are not restrictive and could be effective retroactive to the first day of the COVID-19 public health emergency declaration. Previously, revised BHP Blueprints could only be submitted prospectively.
CMS sets and enforces essential quality and safety standards for the nation’s healthcare system. It is also the nation’s largest health insurer, serving more than 140 million Americans through Medicare, Medicaid, the Children’s Health Insurance Program, and federal Health Insurance Exchanges.
These actions, and earlier CMS actions in response to COVID-19, are part of the ongoing White House Coronavirus Task Force efforts. To keep up with the important work the Task Force is doing in response to COVID-19, visit www.coronavirus.gov. For a complete and updated list of CMS actions, and other information specific to CMS, please visit the Current Emergencies Website.